

Blog post
Research: Health literacy and health disparities in southeastern North Carolina
As a researcher, I ask, "Why do these disparities exist and what can we do to narrow the gap?"

In the United States, kidney failure affects communities of color at higher rates than whites. Higher disease rates and poor outcomes for chronic conditions in these groups is a problem that has concerned the medical community for decades.
As a doctor, I work to provide the highest quality medical care possible to these people. As a researcher, I ask, "Why do these disparities exist and what can we do to narrow the gap?"
In North Carolina, health disparities are even greater in the southeastern counties, where the rates of kidney disease are among the highest in the country. Here, people of color are twice as likely to die from kidney disease or to develop kidney failure.
With a grant from the American Kidney Fund's Clinical Scientist in Nephrology Program, we are studying ways to prevent and improve outcomes for kidney disease in southeastern North Carolina, with an initial focus on Robeson County.
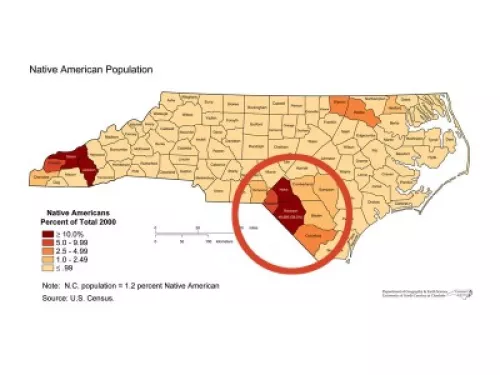
The counties in southeastern North Carolina are among the poorest in the United States. As such, their residents suffer several economic, social and structural barriers to achieving good health outcomes. In Robeson County alone, where 40% of the population is American Indian Lumbee and 30% is Black, the mortality rate for diabetes, kidney disease and heart disease is more than twice the state average.
Many individuals in these groups experience high social, emotional and economic stress throughout their lives. Prolonged and accumulated stresses can lead to higher rates of disease and poor outcomes for chronic conditions like kidney disease because people under stress often have limited coping skills, are not good at communicating with caregivers and doctors and have lower health literacy: the ability to obtain, read and understand and use health care information.
We believe that by studying health literacy, self-care behaviors, self-confidence, stress and coping, social support and self-management skills related to kidney disease, we can improve long-term health outcomes because:
- Health outcomes are improved by modification of self-care behaviors, such as eating, lifestyle and self-management skills like communication with caregivers and taking medication as prescribed
- Inadequate health literacy has been linked with poor health outcomes for chronic conditions
- Structural barriers at the community and neighborhood level are important determinants of health
- Previous work has shown that interventions based on comprehensive assessments of these individual- and community-level factors can improve health outcomes for chronic diseases, including kidney disease.
By identifying how and why these factors are associated with poor outcomes for kidney disease, we will eventually be able to develop interventions that are tailored to the population in our study, but are broad enough to improve health across the region, and nuanced enough to address critical differences among the racial/ethnic populations. We consider this to be the beginning of a sustained effort in the region to address these health disparities related to kidney disease. With the generous support of the American Kidney Fund's Clinical Scientist in Nephrology Program, we are now positioned to develop a long-term public health agenda to achieve these goals

Related articles

Blog post
Junelle Speller, chief strategy officer at the GlomCon Foundation, describes how the organization is working to increase awareness of AMKD

Press release
Program addresses gaps in kidney-specific education for frontline professionals to help with prevention, detection, education and care coordination of kidney disease.

Press release
Symposium will highlight AKF's work to advance kidney health equity through its Kidney Health for All® initiative

Blog post
AKF awarded 12 organizations and 36 coaches with grants in the fourth year of the KHC Health Equity Grant program
